Presbyopia Virginia, Maryland, and Washington, D.C.
Description
Dr. Andrew Holzman explains his practice’s process of strict screening for good candidates to undergo LASIK eye surgery. Even if patients have good eyesight, the eyes’ lens will weaken down the road, and eventually people will develop presbyopia. Dr. Holzman’s ophthalmology practices in Virginia, Maryland, and Washington D.C. can help correct your vision issues.
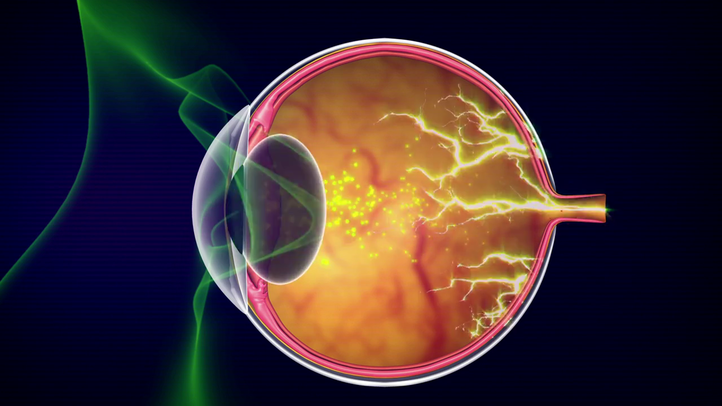
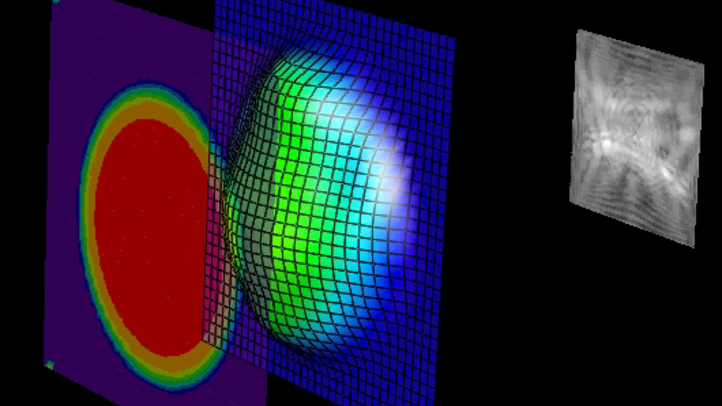
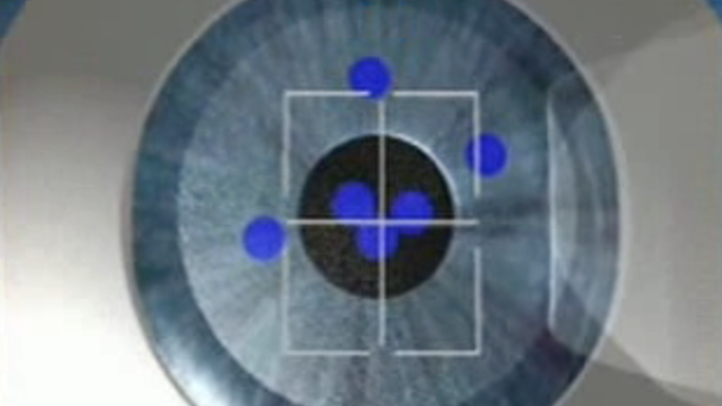
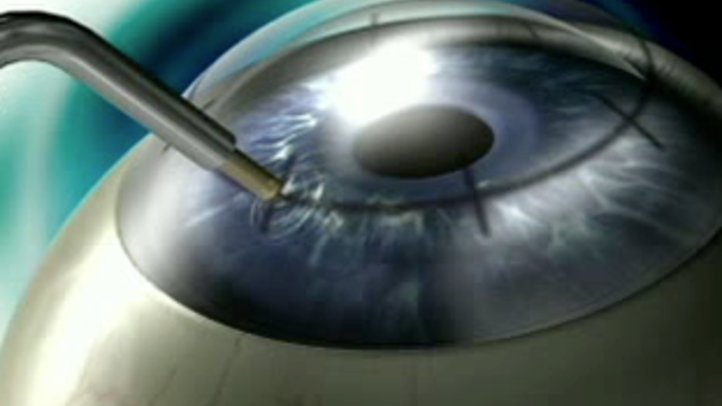
DR. ANDREW HOLZMAN: Welcome to TLC Tysons Corner, folks. I’m Dr. Holzman, and today we’re going to do a seminar. It’s the same seminar we do kind of weekly. And the idea behind it is just kind of a casual discussion for you. You’ll get to ask questions of a surgeon and it’s usually very informative. It moves rather quickly. After we’re done with this you’re going to go back into the rooms, individually, of course. We’re going to do a lot of testing on you. We’re going to determine whether you’re a good candidate for the procedure today. We’re going to have you meet with the counselor. So there’s a lot of steps that you’re going to go through today. And hopefully, you’re all going to be great candidates and you’re all going to be happy patients of ours. So this first step I apologize for the group seminar discussion. Some people don’t like group seminars, but it actually helps sometimes for you because somebody might be thinking of a question to ask that you might not have been thinking about. So it is very casual. Feel free to ask questions as we go along. And I’m a big believer in education before the surgery so I think it’s really important information that you know this stuff and hopefully, you’ll get something out of this. I am a corneal specialist. A corneal specialist of course, I’m a board-certified ophthalmologist, of course, you have to be a board-certified ophthalmologist to do this, but I went on for extra training and took a fellowship in corneal surgery. So this is a cross-section of the eyeball. And you’ve got the front and the back. And the front of the eyeball is called the cornea. It’s actually the window of the eye, okay? So what we’re doing in these procedures is we’re changing the shape of the window of the eye. So all we’re doing is changing the shape of the cornea. We’re not dealing with the internal mechanisms of your eye at all, okay? So it’s just a very kind of superficial treatment changing the front window shape. The fact that I’m a corneal specialist is a good thing. This is corneal surgery. It separates me a little bit from the rest of the pack of docs that do LASIK. And for that reason we get a lot of referrals from other places, outside places, because of my corneal expertise. So it is a little bit different in that regard. Now, in terms of the seminar, we do this to educate patients. I don’t think you need motivation. You’re sitting here so hopefully, you’re motivated already. And we want to do this to answer questions and provide some interaction for you. You might be amazed that 20% of patients that come in this door are turned away. Now it varies very much based on the month. Some months it’s 15% and some months it’s 20%. Some months it’s 25%. But we’re a very conservative center. So you have to understand, we’re not going to operate on you unless we think that you’re going to do well. Okay? It’s very simple. We want to eliminate a lot of the risk, or most of the risk before we start the surgery. So by doing so, and being very conservative and telling patients you’re not a candidate, every time I sit down to operate I feel like I know the patient’s going to really well. Cause I just, you know, because of our experience and the state of the art equipment we have, and the fact that we’re operating on excellent candidates, it means that you’re going to do well. And it makes it allows me to sleep well at night knowing that. So you can rest assured that we’re not going to operate on you unless you’re a perfect candidate for this procedure. And that’s very important. Information on me is basically I trained up and down the east coast and I moved here about 11 years ago to open this center and have been doing refractive surgery for 20 years. So I’ve been doing this since 1991. I’ve done over 50,000 procedures. And that’s a lot of surgery. So I’ve seen a lot of things over the years. I’ve been with refractive surgery since the beginning. We were doing radial keratotomy years and years ago, and you might remember what that was. And we were using diamond blades and things like that. So it’s evolved tremendously to today, and it’s at the pinnacle of I can’t it’s just an absolutely fantastic procedure to have done today. Very, very safe and very effective. Who has it done? Well, we do a lot of occupational therapy at this center. We do a lot of military, we do a lot of pilots, we do a lot of FBI, we do a lot of firefighters. These are people that require good vision for their jobs. What I’m most proud about is that we do a lot of eye doctors’ eyes. I’ve done at least 30 or 40 local eye doctors’ eyes in the community. Certainly they know where to go if they want to have their eye surgery and they come here. So I’m very, very proud of that fact, and I’ve operated on many, many more of their family members. So that’s something that I’m kind of proud of. But you’re probably here because you can’t tolerate glasses or contacts, and that’s the most common reason. And you have a refractive error. That’s what makes you need to wear glasses or contacts. So you are either nearsighted or farsighted with astigmatism, okay? And some of you have a lot of astigmatism and some of you have a little bit, but most of you have some. And what nearsightedness is, is you take your glasses off and you can see it near, okay? It’s appropriately named. So you take your glasses off, you see something you close, but you can’t see the world. It’s all blurry out beyond this point. And that’s because your focal point is right here. Or right here, if you’re really bad, okay? Which some of you might be. So the problem with nearsightedness is that the cornea is too steep. So the corneal dome sticks out a little too far. And when you look at a distant street sign let’s say it’s this object out here, a street sign it’s focused right inside the jelly of the eye and it needs to fall on the back wall of the eye in order for you to see it clearly. So what you’re doing is wearing glasses or contacts in the front, which are just basically pushing the image of the street sign backwards so that your brain can see the street sign. And that’s how your glasses work. What we’re going to do is we are going to flatten the dome just to the appropriate amount for your particular eyes and when we do that we’re going to be able to move the street signs image backwards onto the back wall of the eye, okay? So it’s just like you’re wearing your glasses or your contacts, but you’re not, okay? Astigmatism is a term that basically means that you have a curve in your cornea, okay? So the front window of your eye is curved a little bit more than average. So it’s not as perfectly round as it should be. So what we’re going to do is we’re going to reshape that at the same time we’re treating your nearsightedness so that the curve is no longer there. And so it’s more round. Farsightedness is the opposite problem. People who are farsighted, their corneas are too flat, and look at where the street sign ends up it’s behind the wall of eye. Okay, so what we have to do is the opposite. We have to steepen the corner and move their street sign image forward, okay? So these are all treatable with the LASIK, okay? Now, one thing I want to mention at this point most people are always wondering about me because I’m pretty much the only one in the room not wearing glasses. And they always well, did you have eye surgery? Did you have LASIK? And the answer is I’ve always had good eyesight, okay? So I’ve never needed LASIK and I don’t need to wear glasses or contacts; I just see well, okay. But I’m telling you this for a reason because we’re going to get to the next slide and you’ll understand why I’m telling you this. No matter whether you’re like me and you see really well, or you’re like yourselves, nearsighted with astigmatism, when you get Internet your forties you’re going to develop a condition called presbyopia. So everybody gets this condition. It doesn’t matter whether we’re young or a young nearsighted person or a young farsighted person. When we get into our forties we’re going to develop presbyopia. What happens? Well, inside the eye there’s a lens. And you can think of this sort of like the lens of an autofocus camera. When you take a picture of something, you can take a picture of a distant object with your camera or you can take a picture of a close object, and the lens inside there is going to autofocus for that particular zone that you’re taking the picture in. So with the eye it’s the same thing. Take me, for instance. I see really well. I look at something at a distance. I go to read something. My lens has to reshape itself just like the cameras to see up close. And so when that happens I can read, okay? Now, if I’m in my forties, which I am, my lens starts to weaken. So the autofocus starts weakening. And I’m no longer able to just easily read when, you know, my lens is no longer able to easily change shape, so it’s harder for me to read. So eventually we start holding things a little further out and eventually your arms are too short; you can’t hold it far enough and you have to go to the magnifying glasses. You go to CVS and you buy a pair of reading glasses. So that’s what’s going to happen to all of you. Okay, this looks like a young group so this is boring conversation right now, but when you do get into the forties you will need to deal with reading glasses. It’s not because you had LASIK. It’s because you developed presbyopia. It’s an age-related condition. And it continues to worsen from the point where 45 until where we’re 65. So it keeps getting worse. And there’s really no cure for this right now. However, if you were over 40 and you were interested in having LASIK and you did not want to go right to wearing reading glasses from the drugstore there is an option. And the option is called monovision. And what monovision is, is it deals with the fact that one of our eyes is more dominant over the other. So in my case, it’s my right eye. It’s my dominant eye. So I would take a picture or shoot a camera with my right eye, or shoot a gun with my right eye, okay? So what we would do is we would fix the right eye the non-dominant eye for 20/20, for distance, and then we would leave the other eye a little bit nearsighted so it could read a menu. And so you’ve got one eye seeing better at distance and one eye seeing better at close and that two eyes together work rather well together usually. You can test this out for patients before the surgery. And usually that seriously decreases the patient’s need for reading glasses. Okay. So that’s something called monovision. Now we don’t do that on pilots and we don’t do that on surgeons, but on people who are just kind of, you know, want to decrease their dependency on reading glasses. We do that.